




What are the Causes of DCM?
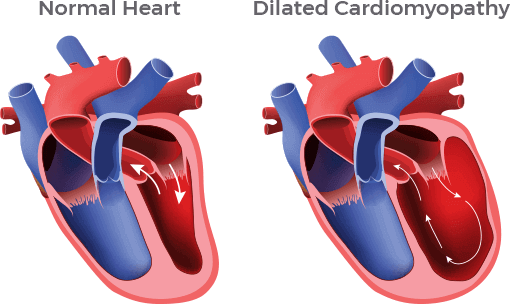
What are the Causes of DCM? About 50 to 60% of all dilated cardiomyopathy (DCM) in the U.S. results from heart muscle damage caused by myocardial infarction (heart attack) from coronary heart disease. Coronary artery disease is a condition in which the blood vessels that provide blood supply to the heart (coronary arteries) become narrowed with cholesterol plaque. A heart attack occurs when a cholesterol plaque ruptures in a coronary artery and blocks the flow of blood and oxygen to the heart muscle. The lack of oxygen (ischemia) results in the death of part of the heart muscle. When a large part of the heart muscle dies from a heart attack, the remaining heart muscle weakens (cardiomyopathy) and the heart may become enlarged over time. This type of DCM is specifically called ischemic dilated cardiomyopathy.
The next most common type of DCM (40 to 50%) is called idiopathic dilated cardiomyopathy (IDC). Idiopathic means “cause is unknown.” For a patient to have a formal diagnosis of IDC, coronary heart disease should have been excluded. Other potential, less common causes of dilated cardiomyopathy should also be excluded. These include certain chemotherapy drugs used to treat cancers (toxic cause), problems with heart valves, congenital heart disease, insufficient thyroid hormone levels (metabolic cause), infection, or iron overload in the heart muscle (another inherited problem).
Individuals with DCM of unknown cause (IDC) do not present a different set of symptoms than individuals with DCM from other causes. They do not present at a different age than individuals with DCM from other causes either. While the symptoms and age of onset of IDC is not different from other causes of DCM, it is now known that genetics plays a role in IDC.
DCM can be a Family Affair
IDC can run in families. When IDC is present in two or more family members, the term Familial Dilated Cardiomyopathy (FDC) is used. Until the early 1990’s, it was thought only about 1 to 2% of cases ran in families. In 1992, however, a U.S. study demonstrated that 20% of patients with IDC had affected first-degree family members (parents, siblings, or children). Data published in 1998 from two European studies reported that 35 to 50% of IDC cases were familial. During the past 20 years, familial DCM genetic studies have identified mutations in more than 30 genes. Most people with a genetic cause of their DCM will have an initial diagnosis of IDC.
Pregnancy and DCM
Peripartum cardiomyopathy (PPCM) or pregnancy-associated cardiomyopathy (PACM) are terms used to describe the onset of DCM of unknown cause that occurs during pregnancy or the first several months in the post-partum period. There may be genetic causes for the development of PPCM or PACM. It is recommended that anyone diagnosed with PPCM or PACM follow the same Screening Recommendations for DCM: pregnant women who have a first-degree relative with idiopathic DCM should be evaluated for the possibility of DCM onset in pregnancy or soon after delivery. Similarly, first-degree relatives of women with PPCM/PACM should undergo cardiovascular screening.
Click to Explore: