

Receiving a DCM diagnosis can feel overwhelming, but you are not alone. While this news can be a lot to process, it is important to know that with modern treatment, most people diagnosed with this condition live long, active, and fulfilling lives.
It’s natural to feel a range of emotions right now. Give yourself permission to process this news at your own pace. This page is designed as a starting point you can return to whenever you’re ready. We are here to help you navigate this, one step at a time.
What is DCM?
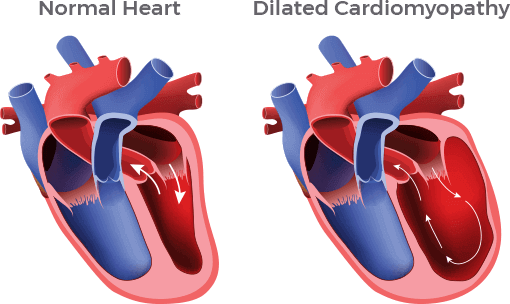
Dilated cardiomyopathy (DCM) is a heart muscle disease where the heart’s main pumping chamber (the left ventricle) becomes enlarged, or “dilated.”
What happens?
As the heart stretches, the muscle walls become thinner and weaker, making it harder to pump blood efficiently.
How common is it?
DCM affects approximately 1 in 250 people.
Who gets it?
It is most often diagnosed in adults ages 20–60, but it can develop at any age.
Translating the medical terms: A DCM diagnosis comes with many new terms. It’s normal to feel like you’re learning a new language. We have created a Glossary of Terms to provide simple definitions for the heart health vocabulary you will hear from your care team.
What are the Common Causes of DCM?
Identifying the cause of DCM can guide your doctors in choosing the most effective care plan.
Most cases of DCM fall into one of two main groups: primary or secondary.
Primary
(Something intrinsically abnormal about how the heart muscle functions)
Secondary causes are ruled out, and patients are often given the diagnosis of idiopathic DCM, meaning that the cause is not known. We now know that many, if not most people, who fall into this category have a genetic cause for their DCM.
Secondary
(Caused by another disorder or disease)
Causes include, but are not exclusive to, ischemic heart disease, valvular heart disease, severe hypertension, inflammatory causes, toxicities (e.g., certain chemotherapies), tachycardia mediated, metabolic, and nutritional deficiencies. Of these causes, ischemic heart disease is the most common in the Western world.
Familial (Genetic) DCM occurs when two or more family members have idiopathic DCM. First-degree relatives (parents, siblings or children) have roughly a 50% chance of carrying the same genetic marker. Identifying genetic mutations can guide treatment and future therapies.
Pregnancy-Related DCM (Peripartum Cardiomyopathy, PPCM) develops during or shortly after pregnancy. There may be a genetic link, so women with PPCM and their first-degree relatives should follow the same cardiovascular screening guidelines as those with genetic DCM.
To learn more, visit Causes of DCM.
What are the Common Symptoms of DCM?
When your heart struggles to pump blood because of DCM, fluid can sometimes build up in your body. Your doctor can help manage these symptoms.
Early warning signs of DCM include:
Shortness of Breath
Difficulty breathing while resting or lying flat.
Activity Limitations
Getting winded during simple tasks like climbing stairs.
Edema (Swelling)
Puffiness in your legs, ankles, or abdomen.
Fatigue
A constant feeling of being “worn out,” even after rest.
To learn more, visit Heart Failure Symptoms.
How is DCM Diagnosed?
Your medical team typically uses three primary tools to establish your “baseline” health. These tests help your doctors understand how your heart is working right now so they can track your progress over time.
Common diagnostic tools include:
Echocardiogram (ECHO)
An ultrasound that images your heart to check its size and pumping function, known as Ejection Fraction (EF).
Electrocardiogram (EKG/ECG)
This records your heart’s electrical rhythm to detect irregular beats (arrhythmias).
History & Physical
This is a deep dive into your personal health journey and family history to identify genetic risks or external triggers.

Know Your Numbers: Ejection Fraction (EF)
Ejection Fraction (EF) is the percentage of blood pumped out of the heart with each beat.
Normal EF: 50%-65%
Borderline or mildly reduced EF: 41%-49%
Reduced EF: 40% and less
This is where medical treatment and monitoring are most important to support better heart function and outcomes.
To learn more, visit Heart Function & Tests
Screening & Genetic Testing
If your DCM isn’t caused by a heart attack or coronary disease, it is often linked to genetics. Because cardiomyopathy can be “silent” (present without symptoms), screening and testing are powerful tools for early detection to protect both you and your family.
Should I Get Genetic Testing?
Major medical organizations, including the AHA (American Heart Association) and ACC (American College of Cardiology), recommend genetic testing for anyone with DCM with an unknown cause or family history of cardiomyopathy.
Identifying a genetic mutation can be lifesaving because it:
Guides Your Treatment
Knowing if a specific mutation caused your DCM can help your doctors tailor care to your needs and improve outcomes.
Identifies Family Risk
Children and siblings of someone with genetic DCM have a 50% chance of inheriting the same mutation. Testing clarifies who is at risk and who isn’t.
Contributes to Research
Your information can help scientists better understand genetic DCM and support ongoing research that may lead to new insights and potential future treatments.
To learn more about genetic testing, the process, and what it means for you, visit Genetic Cardiomyopathy Awareness Consortium (GCAC).
Outlook & Treatment
DCM is typically a chronic condition, meaning it is something you will manage for life. While there is currently no “cure” that restores the heart muscle to its exact state before diagnosis, the outlook for people with DCM today is brighter than ever.
Restoring Your Quality of Life
With a consistent treatment plan, many patients are able to return to their daily activities and feel very close to how they did before their diagnosis.
Key Elements of Your Treatment
Medications
These are the foundation of your care. They reduce strain on your heart, manage fluid, and support heart recovery by helping it pump more efficiently.
Heart Devices
If medications alone aren’t enough, your team might suggest devices like pacemakers or ICDs (defibrillators). These help maintain a steady rhythm and protect your heart from dangerous electrical changes.
Tailored Care
Your plan is unique to you. Whether your DCM is genetic or acquired, identifying the cause helps your care team choose the most effective approach.
Proactive Management
You are the most important member of your care team. Heart-healthy nutrition, staying active, and maintaining a positive mindset all contribute to better long-term outcomes.
Future Hope
For those with DCM due to a genetic cause, we have hope that emerging gene therapies will one day provide even more targeted ways to manage or treat your DCM at its source.
DCM Treatment Milestones:
Discover how treatments for DCM have evolved over the past 60 years and why there is real hope for patients today: DCM History & Milestones

A Vital Note on Treatment
Without medical intervention and regular doctor visits, the prospects for long-term health are significantly lower. Staying consistent with your care team visits and your medication schedule is the most important thing you can do for your future. These are the keys to long-term health and better outcomes.
How Much Improvement to Expect?
While every case of DCM is unique, the majority of patients who follow their treatment plan see significant improvements in their health and quality of life.
Long-Term Success
By avoiding known risk factors (like smoking or excessive alcohol), and staying active, many patients live long, happy lives that are not defined by their diagnosis.
The Goal of Treatment
With consistent medication and follow-up care, many patients see their heart function improve, and their symptoms decrease. In some cases, the heart can actually “remodel” itself, becoming stronger and more efficient over time.
Advanced Options
For patients with more severe cases, modern medicine offers advanced interventions. This can include specialized heart devices or, for some, the possibility of a heart transplant.
You Are Not Alone
It is important to know that you are not alone! There are many online resources that can assist DCM patients and their family members feel more hopeful and supported through this journey.
View Support Groups & Resources